Achilles Pain
What is it?
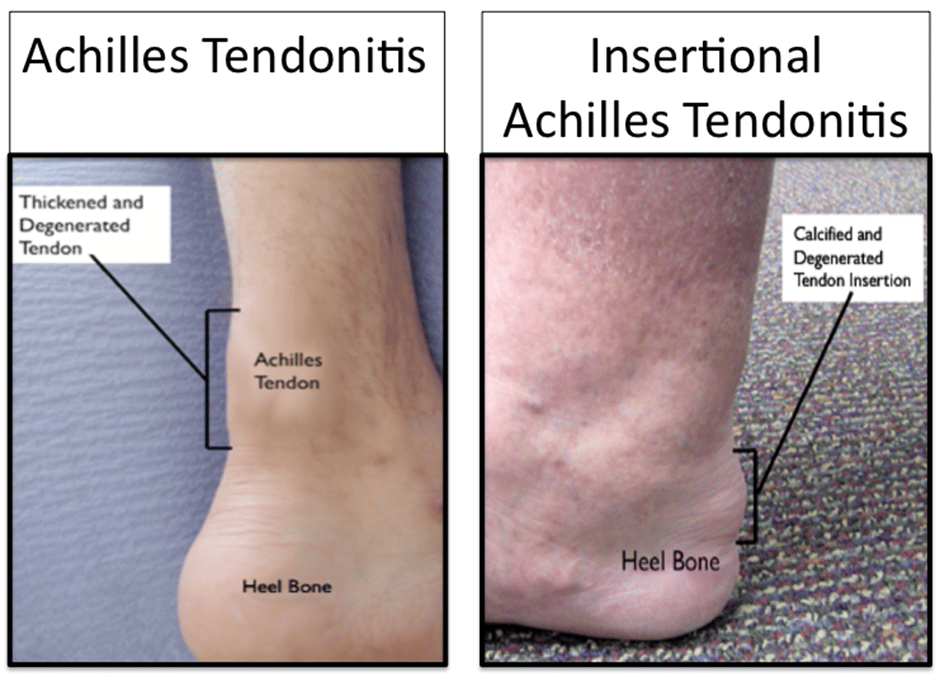
Achilles pain can be either at its insertion on the heel bone or a lump in the middle of the tendon. Insertional pain is usually accompanied by a bony lump known as a “pump bump”. In the middle of the tendon there is usually a painful swollen lump that affects mobility and sports.
I carefully assess where in the Achilles the problem is and also whether it is the tendon itself or the surrounding structures as the management is subtly different depending on where the problem is.
What causes it?
Midsubstance Achilles pain is related to overuse and tight calves and usually affects active people. It can be avoided by regularly stretching your calf muscles. Insertional pain is more of a wear and tear condition that is more likely if you are heavier or when you get older.
How can I treat it?
My first aim is to have a clear diagnosis and come up with a clear rehabilitation plan. For mid-substance pain stretching exercises are best, whereas for insertion pain stretching can make the pain worse and gentle strengthening is better. For both conditions, if the symptoms are not settling with appropriate therapy, I will ask my specialist foot and ankle physiotherapists to offer you a course of shockwave therapy.

What does surgery involve?
For mid-substance Achilles tendinopathy, I prefer to take a stepwise approach to surgery. If all conservative measures have been unsuccessful, the first stage is a mini-open muscle release to give the Achilles some stretch, accompanied by a percutaneous clearance of the tendon from its surrounding structures using a camera through two tiny incisions and an injection of biologic PRP. I feel that this multimodal approach gives you the best chance of a quick recovery.

If this does not work the next stage is a keyhole tendon transfer to make another tendon do the work of the Achilles and take the pressure off of it. Although this is minimally invasive and works well, I feel that wherever possible it is best to try and heal your natural tendon and not weaken other structures.
For insertional Achilles tendinopathy, if conservative measures fail, I feel that the best option is keyhole surgery to remove the extra bone without damaging the Achilles tendon itself. This procedure is preferred as it has less downtime and fewer problems with skin healing.

In redo cases and very severe cases, I prefer a mini-open operation to remove the extra bone and reattach the tendon. This used to have a very long recovery with 6 weeks off of your feet but with modern speedbridge technology recovery is much quicker and you can walk in a boot in 2 weeks.

Aftercare
For all Achilles procedures, you will be non-weight bearing in a cast for 2 weeks followed by 4 weeks in a boot with progressive strengthening with the therapists. Depending on the procedure you will return to full activities between 4-6 months.
Risks and complications
There are risks to all surgery and conservative measures should be tried when possible. If surgery is an option, we will discuss all of the pros and cons and the risks that are specific to you in detail.
The main risk of Achilles surgery is wound problems which is why I try and use minimal incisions wherever possible. It is also important to keep in mind that with appropriate physiotherapy and shockwave most patients do avoid surgery.