Painful Big Toe
What is it?

Pain in the big toe is generally caused by damage within the joint between the big toe and the foot. Other causes of pain in the big toe can be an acute swelling of the big toe such as in gout or a problems with the sesamoids.

The sesamoids are small bones under the big toe that work in the same way as your kneecap. Damage to these bones can be subtle and is something I always look out for when assessing your big toe.
Why does it happen?
Damage can be age-related wear and tear, suffering from repeated bouts of gout, or old injuries to the big toe. However, most cases are partly genetic and run in families. Most people initially complain of pain when the big toe is bent up such as standing on tiptoes or more commonly running but as the condition becomes worse patients can end up in constant pain.
How can I treat it?
The first stage is a careful assessment as to exactly what is causing the pain and if there is wear in the joint exactly how bad it is. There are a number of non-surgical options that can really help in relieving the pain in the big toe and I like to try these first to see if they will relieve the pain for you. As the pain is usually caused by excessive bending of the toe, a stiff insole can reduce the movement and help with the pain, I organise these treatments through a good podiatrist. If the main issue is pain rather than stiffness an injection into the joint can reduce inflammation and my preference for the big toe is a joint fluid substitute known as hyaluronic acid rather than a steroid injection as I feel this is a more natural product. I will explain this to you in detail if it is an appropriate option.

What does surgery involve?
If pain and stiffness are not settling with the non-surgical techniques, I utilise different surgical options depending on the severity of the disease. If the main problem is a lump of bone at the top of the toe and pain on bending, I perform a keyhole bump removal using a small burr.


This is an advance on a well-recognised technique known as a cheilectomy but is much less invasive and allows early movement and stretching which is good for rehabilitation. If the joint is significantly damaged, I consider either joint replacement or fusion.
Joint replacement or joint fusion?
Whilst training in Edinburgh, I published the 15-year results of a randomised controlled trial of joint replacement vs fusion of the big toe. This is the longest follow-up of this type of study in world literature. I found that a successful joint replacement works as well but not better than a joint fusion and failure of joint replacements is more common and can lead to long-term problems.
Having said that, a new type of joint replacement for the big toe has been available for the last 5 years and has very promising results.
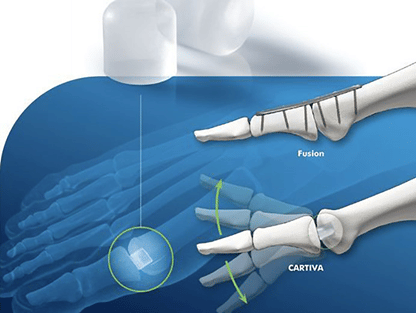
I now offer Cartiva replacement to patients with severe arthritis who wish to maintain a degree of movement in their toe. Although there is still a risk of requiring further surgery this implant is much more straightforward to redo than previous joint replacements and revision rates have been lower than for classic joint replacements.
Fusions still remain the gold standard with reliable pain-free recovery and good function.
Post-op recovery
The recovery after big toe surgery will be dependent on the type of procedure you have (least for keyhole bumpectomy, more for Cartiva, and the most for fusion) but with all procedures, you will be in and out of the hospital the same day and be fully recovered within 3-4 months. We will discuss your recovery in detail and I will give you a personalised plan for your rehabilitation depending on what you want to achieve.
Risks and complications
There are risks to all surgery and conservative measures should be tried when possible. If surgery is an option, we will discuss all of the pros and cons and the risks that are specific to you in detail. Specific risks of this procedure are:
- For keyhole surgery, the main risks are skin damage from the burr and damage to tendons. This is uncommon and the techniques are performed with the specific aim to avoid these complications.
- For Cartiva the most common complication is ongoing pain and the requirement for revision to fusion. This is in about 10% of cases at 5 years.
- For fusions occasionally they do not heal leading to having to redo the procedure. I use strong fixation with screws and a low-profile plate to minimise this risk.